
When people say they want to live longer, they often mean they just want a pill to make them younger. Wouldn’t it be cool? But that’s childish fantasy. If you want to live a longer life — or, more importantly, a healthy vibrant life starting now and live longer with good health, there really are things you can do. It starts with getting your house in order. I’ll include some examples of what I do.
This is long, but I guarantee that if you have a problem in any of the areas below, you will feel better — and live longer and healthier — by fixing it than if you don’t.
This is part of a series: see the index of installments for more.

“Can’t I just take a pill?” Maybe. In the future, probably. The question is, will you die before you can get your hands on it? (See Don’t Die in the Next Five Years.) Meanwhile, you absolutely can reduce damage to your body and feel better starting today. The idea isn’t to live forever in decrepitude, but to lengthen your middle years so you can be active and feel good and get more out of life today!
So what can you do now to increase your chances of living long enough to get there and, in the meantime, have more health and vibrancy? You get your house in order: don’t even think about pills until you can check off every one of the 5 fundamentals below, all of which will have dramatic positive effects on your health. And hey: #5 is only three sentences!
#1: Stop Smoking
Don’t fool yourself: while there are occasional examples of someone living into their hundreds while smoking every day, don’t count on it being you. They probably did it mostly by being born to the right two parents, getting great genes that slowed down their aging process naturally. And it’s very likely they didn’t overdo it: maybe they smoked two or three cigarettes, rather than two or three packs, per day.
A three-pack-a-day habit is just that: a habit, not “savoring the flavor.” It’s an oral fixation that is killing you and aging your body faster than normal. You know this is true, so if living longer and healthier is your goal, you know what you do. That includes smoking pot, by the way: there aren’t even filters involved in a joint! There are healthier ways to ingest it.
How I Did It

I’ve never smoked: I saw enough patients with emphysema in my early ambulance years to get the message in my upper teens. By “never” I mean habitually: I “played” with tobacco a little in my teens, but once I understood the realities of COPD — Chronic Obstructive Pulmonary Disease, including emphysema — I stopped playing around.
I’ve never used pot, either. I wouldn’t hesitate to use it if (for instance) I got cancer and needed to settle nausea from chemo. But I would prefer not to smoke it even then.
#2: Get Your Weight Under Control
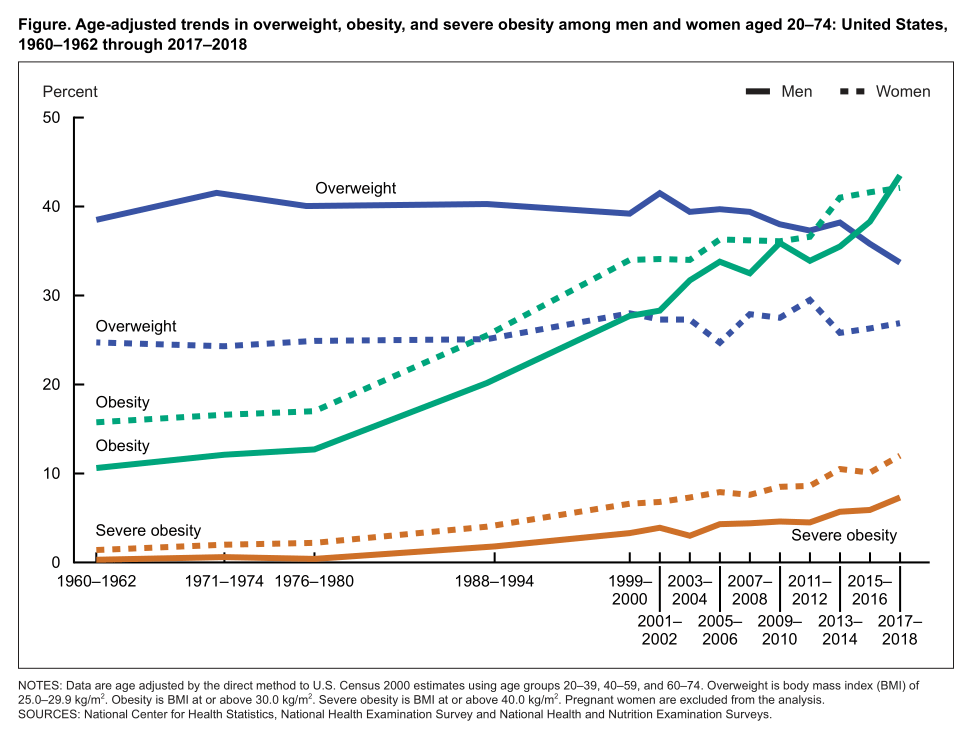
This section is the longest because more than 40 percent of American adults are obese — not simply “overweight” but obese: a body mass index (BMI) of 30 or above. Add in the overweight (BMI of 25-29.9) and that’s more than 70 percent of American adults. Those figures are from a 2017-2018 CDC report; it’s probably higher today.
If you wonder where you are, here’s an anonymous BMI Calculator.
The greater the BMI, the higher the risk for all sorts of health problems that are well known to shorten life and reduce vibrancy: cardiovascular diseases, Type 2 diabetes, obstructive sleep apnea, numerous types of cancer, osteoarthritis, clinical depression (which is a vicious circle: depression often leads to overeating), and, in this day and age, significantly worse outcomes from Covid-19 infections.
Quickly losing weight is hard. If you’re overweight, I don’t recommend a diet.
“Diets” are when you starve yourself for weeks on end with some specific food plan (“paleo”, “Mediterranean”, “South Beach” or others) to reach a specific weight, and then you stop …and gain it all back again, or more.
My vision of myself was that I would never weigh 200 lbs. (91kg) or more: I’m 6ft-3in (1.9m) tall. Interestingly, I found out along the way, 200 lbs. for my height equals a BMI of 25 — the tipping point for clinically overweight.
A few years ago I broke 200, so I “went on a diet” and got under 200 again. Success! Except that sure enough, it crept back up and not only broke 200, I got to a maximum of 202.6 pounds.
Few friends thought I “looked” overweight. But that’s the problem, isn’t it? Let others convince you “oh, it’s not that bad” and it keeps creeping up and up and — uh oh: obese.
I wasn’t going to let that happen to me.
How I Did It
“My name is Randy, and I’m a sugarholic.”
First, if you have a significant weight problem that’s already affecting your health, including being diabetic or pre-diabetic, work with a doctor on this.
Rather than go on a diet, I radically changed my lifestyle. I used to stop at Taco Bell for lunch, and wash it down with a large soda …which I would refill after eating and take it on the road. Taco Bell’s web site says a large soda is up to 420 calories, which is an enormous amount of sugar. (I can’t do “diet” because I have a very bad reaction to aspartame, the usual artificial sweetener.) I went cold turkey on soda; currently, I’ll indulge in 2-4 12 oz. cans of soda per year.
I also cut way back on desserts and candy.
Sugar is really, really bad for us. Rather than write a lot about visceral fat and what it does to you, I’ll suggest you read this article on Wikipedia.
To my utter astonishment, cutting out my huge soda intake cold turkey, and cutting way back on chewable sweets (especially cookies) resulted in …absolutely no weight loss! Worse, my cholesterol and triglyceride levels were still bordering on, and sometimes well into, unhealthy levels.
So what did I do?
A one-two punch forever lifestyle change.
First, in a bit of irony, I switched out sugar for fat. No really: hear me out. In the mid 1900s, government nutritionists told food manufacturers they had to cut down on fat in foods — so they replaced it with sugar. That was a disaster, as shown by the chart above.
Fat, in moderation, is a good thing: in addition to adding flavor naturally, it makes food more satisfying, giving you a “full” feeling that lasts for hours. Sugar, on the other hand, creates a spike in blood sugar, which causes your body to shoot out a big dose of insulin, which results in a blood sugar “crash” …resulting in a craving for more of that sugary food in a fairly short time. See the problem? Worse, over time your body builds up insulin resistance, which is a factor in diabetes.
Kit (my wife), who does lots of research on nutrition, is who convinced me to increase fat intake, by the way.
So yes, I allowed for more fat in my food, especially extra-virgin olive oil (get it from Costco if you can: it’s both good quality and cheap), and avocados, but also some animal fat, of course working to keep it in moderation.
The next spring my doctor was astounded when he saw my blood test results: the “total” cholesterol number (guideline: under 200) went from a high of 223 to 145. LDL (guideline: under 130) went from a high of 160 to 88. Triglycerides (guideline: under 150) went from a high of 275 to 131. Those are pretty radical results.
Without Drugs.
I’m not on any drugs to work on this. It’s all due to switching out sugar for moderate fat, plus what I discuss next. There also could be some effect from supplementation, but I’ll cover supplements in a later installment. For sure I’m not taking any “natural statins” like red yeast rice: I’d much rather do this with food than drugs.
When I told my doctor how I did it, he blinked a couple of times and asked, “So, for breakfast you’ll have three eggs and a rasher of bacon?” Yep, I said, exactly — at least sometimes. He sure couldn’t argue with the numbers — and he could see my weight was going down too.
Second: I was doing intermittent fasting. I began with the method discussed by a British doctor in The Fast Diet *: not eating anything for a 24-hour period at least once, and preferably twice, per week. Aka, fasting, the latter called “5-2” fasting. Water, tea, and coffee OK as long as there were no calories; some say no artificial sweeteners, either.
Sounds rough, doesn’t it? It is …but only at first. After a big meal I’d simply not eat again for 24 hours. For awhile I was naturally pretty hungry before time was up, even though I had enough fuel on board. Yet as my body got used to it, it wouldn’t scream “I’m dying! Gimme fooooood!” — it got easier each week.
I wasn’t fanatical about it: if I burned a lot of energy (say, on an ambulance call), I might feel weak and break the fast early, and endeavor to start over again after recovering for a day. Now and then I fasted three days in a week.
But I later modified it to a “newer” version of fasting that I found much easier: “limited eating window” or “time-restricted eating.” Turns out that’s really good for your body, in part for reasons I’ll discuss in a later installment. Plus, if you combine it with eating less and, especially, cleaner (e.g., a more Mediterranean style), all the better and faster your results.
The idea is to give your system a rest by not eating for at least 8 hours — and preferably 10 or 12 — every day. Essentially forever.
This is easier than you may think because that includes the time you’re asleep. It’s best if your “eating window” is earlier rather than later: don’t eat after dinner. Studies show “Early-Time Restricted” eating improves insulin sensitivity (which is a very good thing), blood pressure, and oxidative stress. If you also concentrate on eating cleaner (and not so much!), you’ll likely lose significant weight. (Here are other recent studies.)
That’s what I did. It’s not a rapid weight loss, but rather a long-term “change your lifestyle” process: I’ve been doing it since 2013 with only occasional breaks. Along the way there were plateaus where I’d be at the same weight for weeks to months, but I kept at it and my weight would suddenly start dropping, slowly, again.
Rather than a 12-hour eating window, one study I saw showed that while there were measurable benefits from a 12-hour window, those benefits doubled by dropping the window to 10 hours — and doubled again with an 8-hour window. What I do: my normal bedtime is midnight, so no calories after 8:00 p.m., and I don’t eat again until at least 11:00 a.m., and usually noon.
I’m perfectly happy with two meals a day during that time, usually noon and around 6:00 p.m. And that’s what caused my weight to drop the most healthy way: slowly.
My Results: Over several years of sticking too this one-two approach, I lost more than 30 pounds, bringing my weight to 168, which translates to a very healthy BMI of 21. These days my weight varies between 168 and 172, usually over the span of weeks.
Bonus Bit: Stop Eating Processed Foods
I used the phrase “food manufacturers” above. Many foods, especially in the U.S., are often made in a factory, not picked fresh and rushed to your grocer or table. Prepared dinners, bags of potatoes prepared for your air fryer (or, horrors, deep fryer!), highly flavored chips, frozen pizza, packaged mac and “cheese” (or the frankenfood disaster called “cheese food” — they can’t call it cheese, but it’s kinda like cheese so it’s “cheese food”!)
For just one example, a recent report found that an additive that’s been in manufactured food since the 1960s — approved because you poop it out later unchanged, so clearly no harm, right? — may have some unnoticed effects on its way through.
Carboxymethyl cellulose (aka CMC, or “cellulose gum”) is added in food manufacturing to add bulk and shelf stability, and it’s true that it comes out essentially unchanged. But more recently, researchers studying the human intestinal biome have found CMC may contribute to “increased prevalence of an array of chronic inflammatory diseases by altering the gut microbiome and metabolome.” That’s not a good thing. And that’s just one of many, many food additives that are are “generally recognized as safe” but may not be at all good for you.
Plus, cutting out frankenfood helps you lose weight.
#3: Get Your Alcohol Intake Under Control
Like food (you have to eat!), this one seems hard because “alcohol in moderation is good for you.” And, like food, if you have an alcohol problem that’s already impacting your health, work with your doctor, telling her you’re very serious about quitting. Because for you, “under control” means stopping. Forever. Especially if you’re a jerk when you drink (e.g., about 75 percent of the obliviots in This is True stories!)

Alcoholism isn’t necessarily any sort of moral failure: the worst of it comes from genetic variations. “The variants with strongest effect are in genes that encode the main enzymes of alcohol metabolism, ADH1B and ALDH2. These genetic factors influence the rate at which alcohol and its initial metabolic product, acetaldehyde, are metabolized.” (More)
I know it’s tougher to quit than this section makes it sound, but if you want to live longer and healthier, get any alcohol problem under control.
For those who don’t have a “problem,” having “some” because it’s “good for you” can easily tip over into “too much” that’s not. The tipping point is certainly at not more than two drinks/day for men, and one for women, but less is probably better.
How I Do It
I’m lucky in that I don’t have a genetic issue with alcohol. I like the flavor, but it’s rare for me to drink much. My consumption averages 1-2 drinks/week (not per day!), and sometimes I can go for weeks without any at all. It helps that I don’t like wine. I’ll sometimes drink beer (usually ales, actually), but it’s rare that I want more than one.
Bonus: fewer calories!
#4: Get Your Blood Pressure Under Control
I talked about this before here, in Luke Perry and Strokes — though having a stroke is only one bad outcome from high blood pressure, aka hypertension. It also is a big risk factor for coronary artery disease/heart attacks, heart failure (which is different from a heart attack), atrial fibrillation, peripheral arterial disease, vision loss, chronic kidney disease, and dementia.
The good news is, the more you get the previous big issues under control, the easier it is to deal with your blood pressure.
Having your BP checked at an annual physical isn’t enough — by far. I highly recommend you get your own BP device because you can’t feel high blood pressure. (If you do, it may be a “hypertensive crisis” which is a good reason to call for an ambulance. But that usually doesn’t cause overt symptoms either.)
Check your BP every day until you get an idea as to in what range it usually is. For that, you need your own monitor. This one is Amazon’s best-selling arm cuff, and it’s well reviewed: 4.7 stars from more than 30,000 people, and under $50.
Wrist cuffs are now quite good, are easier to use, and still accurate (though be sure to keep your wrist at heart level while it’s working). Amazon’s best-seller in that category is this one (under $30, 4.3 stars from 25,000 reviews). The one I have is similar ($25, 4.3 stars/7,000 reviews). The best-seller has one good advantage for the extra $5: it speaks out loud to tell you your blood pressure.
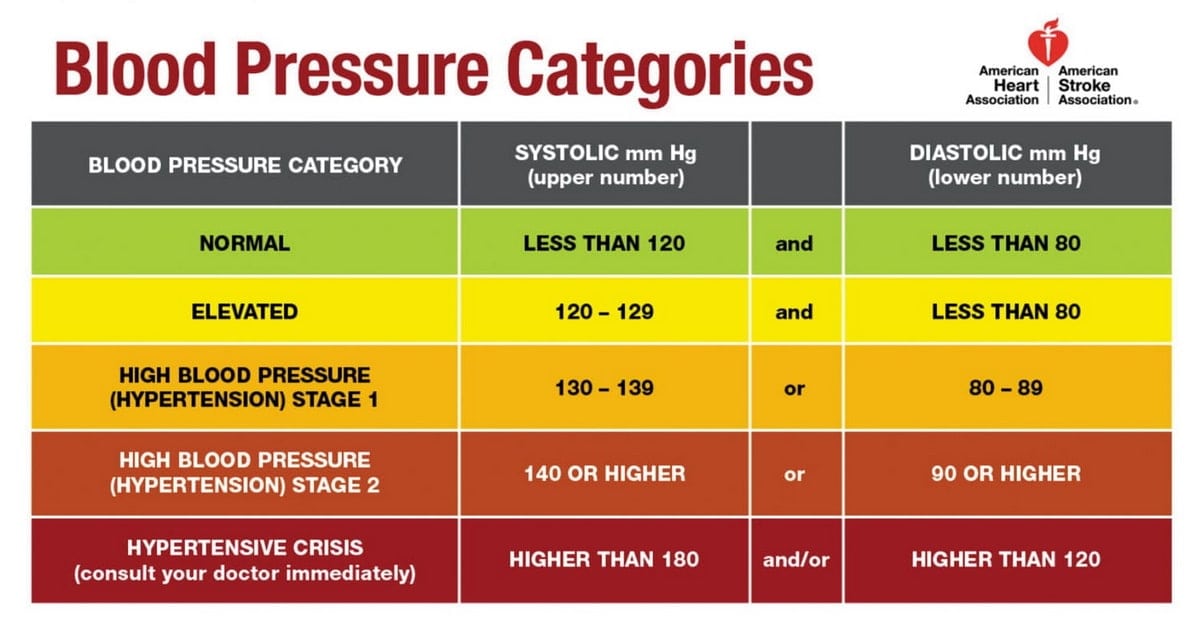
What are you looking for? The first number (systolic) should be under 120; the second number (diastolic) should be under 80. If it’s continually higher than that, see your doctor. If it’s way higher than that (see chart), call your doctor or 911. The 2017 American Heart Association guidelines are still current:
What I Did
I don’t have high blood pressure, in large part because I have all of the above under control. But I had a family member who I would ask about his BP every time he mentioned he had seen a healthcare professional. I kept telling him it was too high, and to bring it up next time he saw his doctor. His doctor put him on meds that helped a little, but didn’t get him into the “normal” range. I kept asking him, but his doctor didn’t think it was an issue — he had been trained under older guidelines.
Then my family member started showing signs of kidney damage — one of the risk factors listed above. He told me his doctor was sending him to a nephrologist — a kidney specialist. “Good,” I said. “I’ll bet he takes your BP seriously!” He sure did: he worked with my family member, trying different drugs until one really worked well, and he is now in the normal range. The lesson learned: keep pushing, since it won’t be your doctor that has the stroke!
#5 (Last): Get Some Exercise
It’s not necessary to join a gym, but if you don’t play any sports or otherwise get exercise, start. A recent study shows you can get good results in as little as 11 minutes per day. If nothing else, walk and stretch!
Conclusion
Obviously “Your results will vary” — but I guarantee that if you get all of these factors in line, you’ll not just be healthier and live longer, you’ll feel better too. And if, later, some new drug comes along proven to make you physiologically younger? Well, you’ll be way ahead of the game, and maybe the extra help will get you to feeling the best you ever have. That’s the idea, anyway!
– – –
Bad link? Broken image? Other problem on this page? Let Me Know, and thanks.
This page is an example of Randy Cassingham’s style of “Thought-Provoking Entertainment”. His This is True is an email newsletter that uses “weird news” as a vehicle to explore the human condition in an entertaining way. If that sounds good, click here to open a subscribe form.
To really support This is True, you’re invited to sign up for a subscription to the much-expanded Premium edition.
Good advice. My mom was a prime example–at 101 she was on no medication, still mentally sharp, and still walking for exercise. After a walk, she laid down for a nap, saying she just wanted to sleep. I tried to call her to wake her up to watch Wheel of Fortune (she still solved some of the puzzles before the contestants did) but she had died in her sleep.
—
What a fantastic way to go! Good for her. My mother is 98 and in about the same shape. -rc
Working on #3 and #5, which should help with #4. I didn’t have to take medication for it until I became obese.
—
Good for you for already working on these! It may seem obvious, but so many just shrug and hope for “a pill.” So great that you’re not starting from zero. -rc
I can’t tell you how many people have argued with me over the years, denying the dangers of the sugar content in “low fat” foods. “This is true”, people!
Good info on the fasting, which I’ve been interested in. I never worked up the will power to fast all day, but I don’t eat until noon, with only coffee (cheating a little with hafnhaf) and a big glass of water in the morning, and generally don’t eat again until after 6pm. My eating issue is I want to snack all evening as soon as the TV’s on, which has nothing to do with being hungry. Lost 25lbs this year, but that’s from riding my bike over 2000 miles (not bad for 68yrs). Still 205lbs though and would like to get below 200. Problem is, winter bike riding goes down and weight starts to inch up.
—
Excellent start. Can you make it a “rule” that you don’t eat past dinner? That may help. My 8:00 p.m. rule has saved me a LOT of calories, not to mention that eating late is particularly bad. -rc
A recent longitudinal study of over 40,000 people associated the highest longevity with a BMI of 27.
While correlation is not causation, the presumed reason was that older people tend to lose their appetite when ill or forget to eat when their memory gets worse. If the person doesn’t have some fat to spare, their body attacks its muscles and organs for sustenance, which can cause already weakened systems to fail.
BMI is also a notoriously inaccurate measure because it’s just a weight to height ratio that doesn’t account for body composition. There are bodybuilders with 4% body fat who are obese based on BMI.
Last, although the AMA successfully pressured Met Life to kill it, their quants briefly published a study in the 80s saying that if you kept your weight relatively stable after 40, your heart has time to develop compensatory strength. Even for the obese, *if they didn’t gain significant weight after 40*, heart issues were not a more significant factor in mortality than it was for people of lower weights.
—
Indeed BMI is a “mass screening” tool. If I was significantly more muscular, for instance, my weight would be >200 in a healthy way, and I wouldn’t worry about it. But it’s not. And don’t put too much weight (no pun intended) on any study that isolates just one factor, like the heart, since to generalize it to health in general is fallacious. Even this page, as narrow as it is, talks about a lot of factors, not just one. -rc
We watched “That Sugar Film” which talks of the amounts of sugar in “low fat” and “natural” products, which impacted us so much we went to the kitchen cupboards and started throwing stuff out (our kids still remember!). I highly recommend watching it as a needed wake-up call, at least it was for me (a sugarholic as well).
I’d add strength (aka resistance) training to the Exercise prescription. Cardio and stretching are fine but inadequate to maintain muscle mass, which staves off sarcopenia. Lots of people are allergic to the whole idea because they associate it with grunting “gym bros” and sticky machines at Planet Fitness, but you can do it with bands or even bodyweight. The key is to keep it brief and intense enough that you go to muscle failure (i.e., you can’t do another rep) after 8 to 12 reps. The good news is that you can start at any age and see improvement, which leads to stronger/denser bones, better balance, and fewer falls — not to mention the ability to get on the floor with your grandkids and carry grocery bags.
—
Totally agree. I’ve seen others put it as “lift heavy things.” Doing planks is also great, as it particularly helps the core muscles, and is zero impact. (For others: sarcopenia is muscle loss that occurs with aging and/or immobility.) -rc
I am *very* intrigued by intermittent fasting. I am very overweight and diabetic. At one point I had learned that it was better to eat 6 times a day, never allowing for more than 3 hours between meals to avoid insulin spikes. Intermittent fasting seems to go completely against that. Is this good even for diabetics?
—
I believe so — but ask your doctor first, or at least research it carefully in the medical journals. I have heard of diabetics not needing insulin anymore after getting control with fasting, but that’s obviously anecdotal. -rc
I am wondering whether “Sleep” should be added to the list? Research shows links to high blood pressure and cardiovascular disease through bad sleeping habits.
—
Yes, sleep is critical. Much of what’s suggested here will help sleep, but indeed too many schedule themselves so there’s little time for it. Big mistake. Then there’s the issue of “can’t” get enough sleep, even when we try. That topic is on tap for a future post. -rc